


When will the Decolonolialists, Antiracists, and DEI People Come for Geriatrics?
An entire movement based on leveraging racialized class envy has seemed relatively slow to make its way to clinical geriatrics, but it won't last.

It seems like over the last several years things have moved extremely quickly in the sociopolitical space.
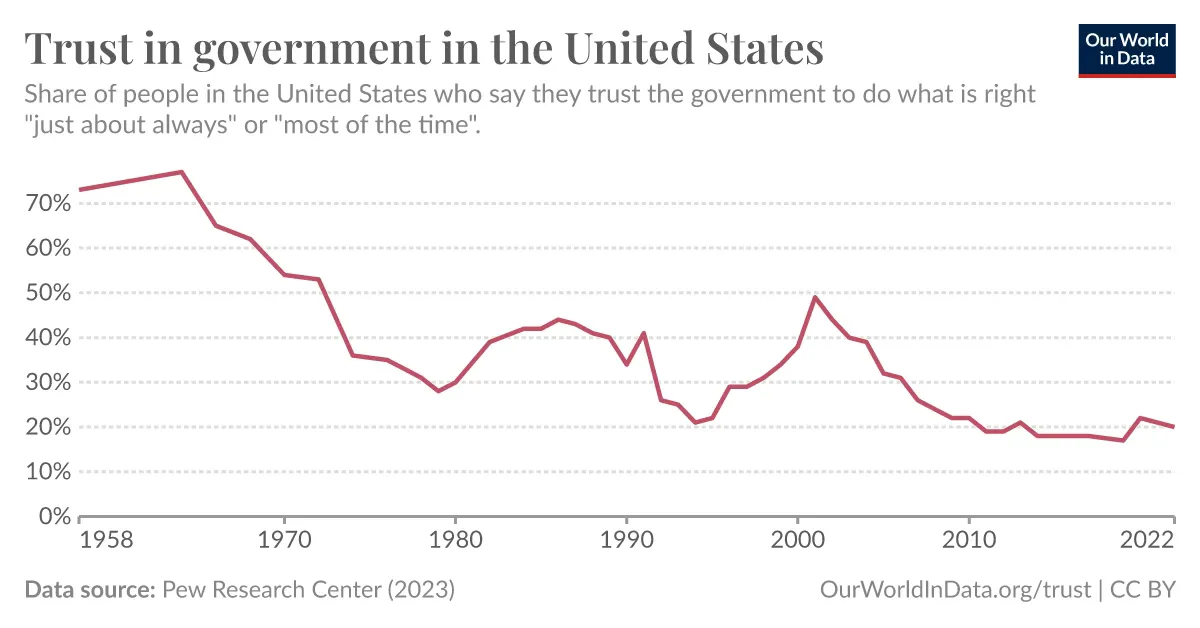
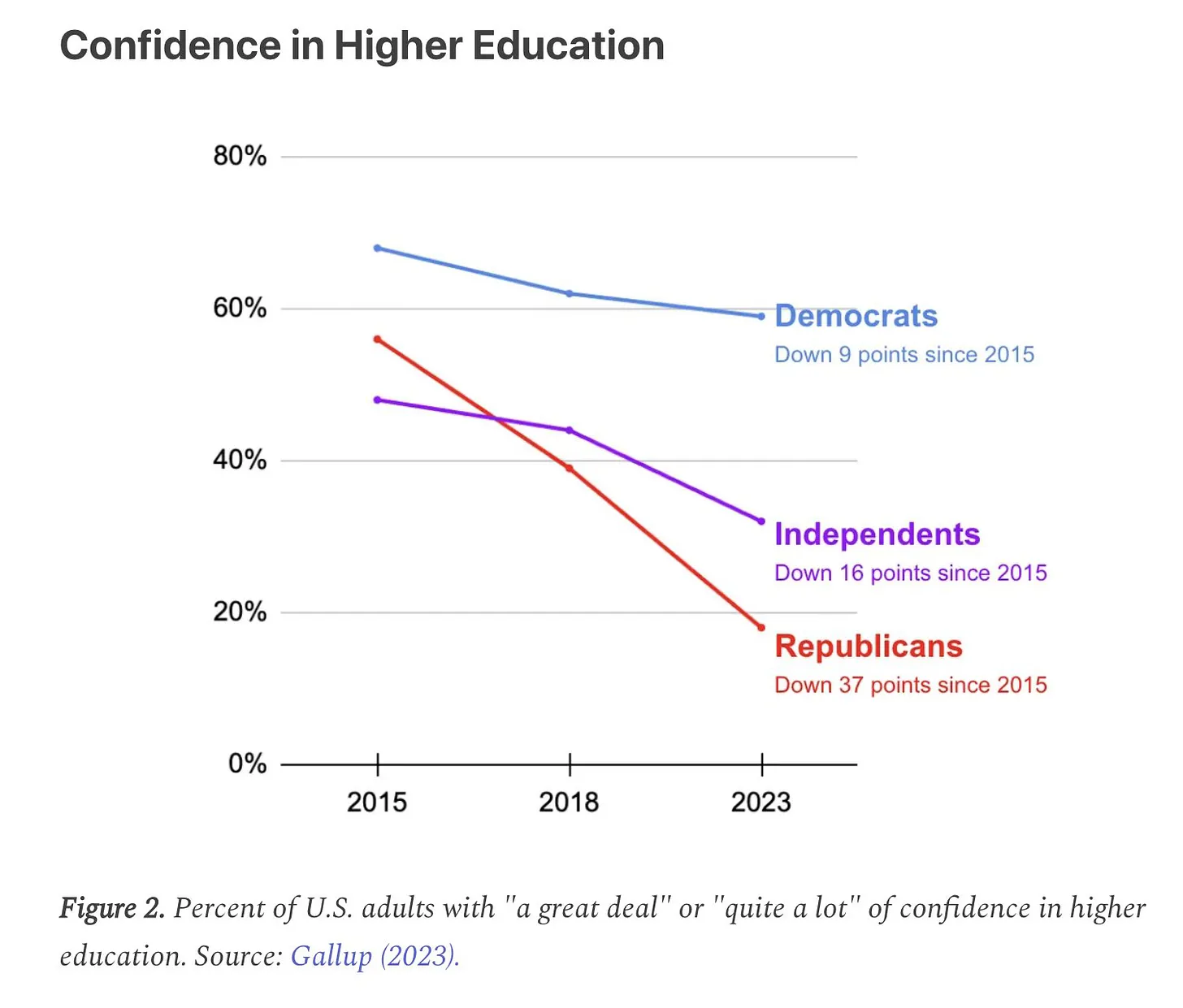
Coronophobia, lockdowns, “mostly peaceful” riots and burning of cities, the wholesale bonfire of credibility of trust in government, trust in journalism, and trust in higher education, the list goes on.
{kind=link}
{kind=link}
{kind=link}
One of the notable trends in institutions has been the wholesale embrace, post-Floyd embrace of what has been popularly called “Diversity, Equity, and Inclusion,” or DEI - which now has massive, multimillion dollar staffing and representation at all manner of corporate, higher education, government, and non-governmental organization (NGO) entities.
No need to spend a lot of time recapping it - I think most people who follow me understand that I see the critical race theory inspired DEI & antiracism movements as nothing more than a rewarming of Marxism (which is where critical theory came from) under a racial lens, although now it includes everything - we have queer theory, feminist critical theory, intersectionality, et cetera - everything is an invisible system of oppression and it must all be dismantled due to it’s “whiteness” and cisheteronormativity. Et cetera.

I’ve been steeling myself for what comes next in the geriatrics and long-term care world, and to be honest, it doesn’t seem like the proverbial shit has hit the fan quite yet.
Yes, for nursing home workers and residents, we have dealt with all sorts of horrors from the CoronaPanic - being forced to ban visitors for months, imposition of the cruel torture of “window visits,” the loss of communal dining, the farcical and abusive spectacle of masking, the list goes on. But many of the more intense versions of these horrors have receded, and although we continue to feel the aftereffects and echoes of the lockdown madness in the form of chronic nursing shortages, and continued absurd regional and seasonal masking policies, and periodic “snap lockdowns,” at least my nursing home is, while not back to normal, at least back to some level of stable functioning.
Recently,
posted this on Twitter / X: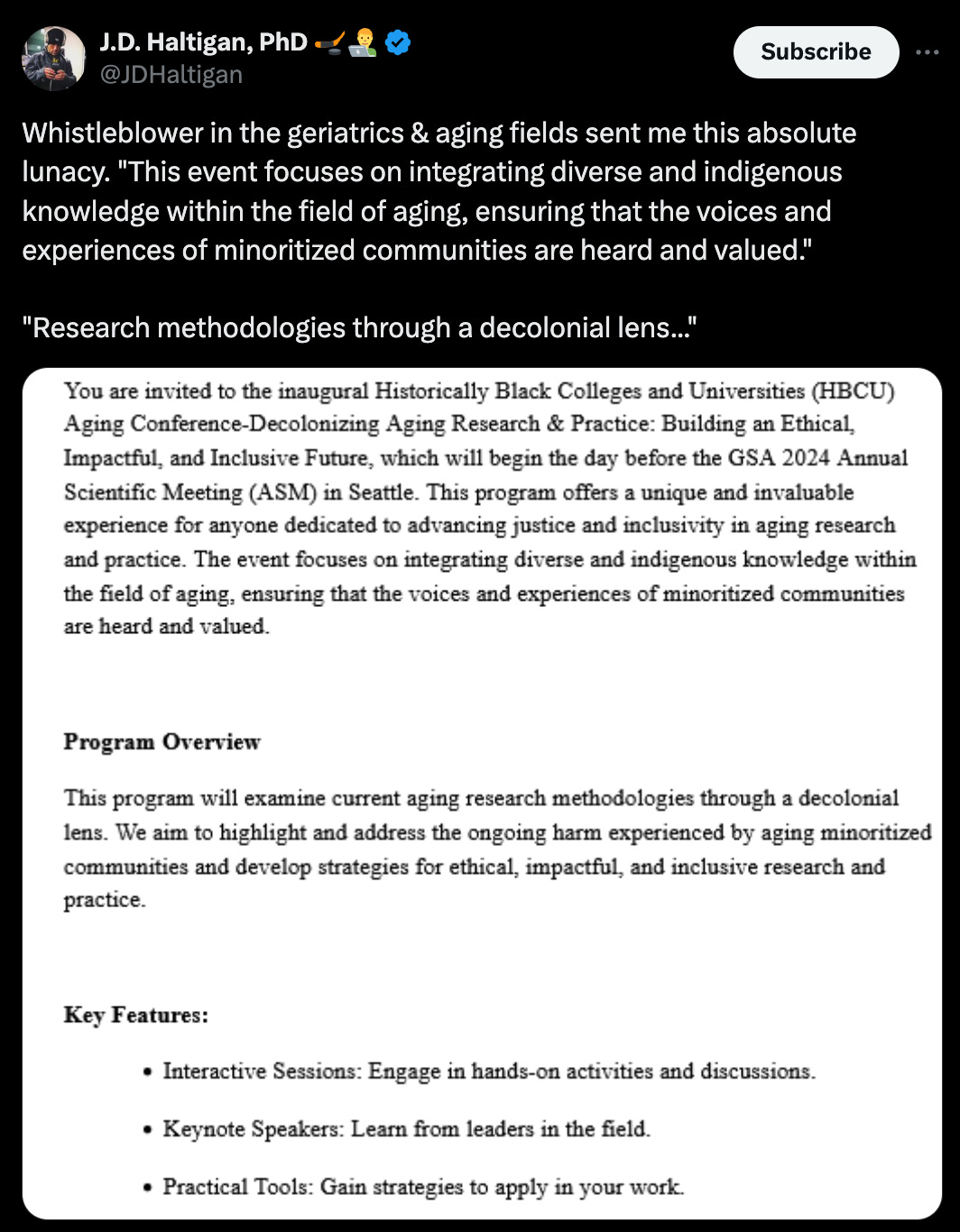
I groaned.
Of course this is coming.
Of course the antiracists and DEI practitioners would be coming for nursing homes, assisted living facilities, family caregivers and their elderly care recipients toughing it out at home.
What would this look like?
At my local hospital system, there was a brief explosion of “antiracist” trainings and continuing education offerings, with new “diversity committees” formed with doe-eyed activists in charge, eager to steer programmatic and ultimately, hiring and retention decisions towards preferred candidates (the constant cacophony of these inane trainings has died down, but the committees remain).
So far - while the COVID assault was relentless and horrible, an absurdly traumatic event for our residents, families, and staff, so far it’s been quiet on that score in the world I operate in.
Why is this? Well, a few things.
Geriatrics and gerontology are not sexy fields. It’s satisfying (and familiar) to the DEI people to wholesale conquer the educational arena like medical schools, colleges, and K-12 schools. They’ve made major inroads in pediatric medical specialty orgs, most infamously the American Academy of Periatrics:

… and have conquered the American Psychological Association:

Groups like the American Geriatrics Society, Gerontological Society of America and other aging related groups have indeed joined the chorus of organizations adopting DEI frameworks, but we have to assess the dangerous implications of the invasion of DEI ideology in the long-term care and geriatrics industry.
The experiences during the COVID-19 pandemic should serve as a cautionary tale. Policies like lockdowns, "window visits," and strict masking mandates were imposed without regard for the profound harm they inflicted on the elderly.
These measures, driven by top-down ideological mandates, prioritized conformity over all else, and resulted in pointless tragedies like this, with the elderly dying alone, only allowed to see their loved ones behind glass:

The DEI push threatens to replicate these failures.
It risks diluting essential standards in healthcare to meet identitarian goals, potentially compromising the quality of care that our vulnerable elderly populations desperately need. In sectors like geriatrics, where the stakes are incredibly high, we cannot afford to prioritize ideological agendas over the well-being of those we serve.
Moreover, the implementation of DEI initiatives in colleges and corporate boardrooms has often led to environments rife with toxicity and dysfunction. Across the United States, we've witnessed college campuses erupt in unrest, with DEI-related policies fueling divisiveness and stifling open discourse.
These environments become mired in conflict rather than fostering genuine inclusivity and respect. Introducing such dynamics into long-term care could be disastrous, creating a workplace culture that detracts from the critical focus on patient care and support.
We must reject any approach that imposes ideological conformity at the expense of effective care. The elderly deserve policies that are grounded in empathy, respect, and a deep understanding of their unique needs—not ones that serve as vehicles for social engineering.
While pluralism and respect for diverse backgrounds are important, the current DEI agenda poses significant risks to the integrity of long-term care. We must remain steadfast in advocating for standards that ensure the highest quality of care, resisting the imposition of divisive and dysfunctional frameworks. Our focus should be on creating compassionate, effective environments where older adults can receive the care and dignity they deserve.
I think it's potentially even scarier than this. As Aaron Kheriaty has pointed out, doctors and nurses didn't just "go along" with the Holocaust, they were at the forefront of it. This happened because they began to believe that promoting the health of the German people (the "volk") was their primary duty, rather than the health of the individual patient under their care. When they began to see certain individuals, such as the demented elderly and the handicapped, as being a drain on the "volk" they initiated a "euthanasia" program....and the slippery slope we are all familiar with ensued.
Kamala Harris (among others) has told us that her goal is "equity" -- not equality of opportunity, but equality of outcome between groups. The AMA and other medical associations are constantly beating the drum of "health equity" -- which means equal outcomes between groups, including racial groups. The Royal College of Physicians and Surgeons in Canada is looking at making this their PRIMARY goal. We have already seen examples of race-based prioritization of certain scarce medical treatments. If our primary goal is to make sure that all races have, say, the same life expectancy, how will we care for an elderly demented white person? Especially if they are also perceived as being "bad for the planet?"
A few years ago, I would have said this kind of thinking was crazy. The COVID debacle taught me otherwise. I wrote about this here: https://pairodocs.substack.com/p/save-the-planet-kill-your-patient