


We Need an Urgency of Normal for Older Adults in Long-Term Care in 2023!
"Urgency of Normal" which successfully stopped the shutdown & masking of public school students and freed them of mandates may not be so easy with nursing homes. But absolutely *needs* to happen.

Update on Environment of Care in My Nursing Home (December 2022)
All of our staff continue to wear masks (because it’s required), as well as face shields on most of them (masks + face shields or goggles still required). Masks are technically required of residents, but I only see them on about maybe a 1/3 of the residents at most.
Community outings with our activities staff have resumed (we had a farmer’s market outing a few weeks ago, a couple of movie outings, and a restaurant outing recently). Masks compliance strictly required for residents on outings.
When residents return, they are required to do a “7 day quarantine” where they are required to stay confined to their room (including for meals) and mask outside of their rooms.
Volunteers have returned in a very limited form. We’ve had a few socially distanced bingo games. We used to have a band visit every Wednesday (a banjo trio plus accompaniments), along with a volunteer-led sculpture class that was extremely popular, but that’s been long gone. We used to have children visit (Boy Scouts, Girl Scouts, etc.) but those are long gone too.
Speaking of children, I don’t recall seeing a child under 15 at my nursing home for the last 3 years, even with families.
Visits still require scheduling with nursing staff. Visits are limited in terms of number of visitors. Families have to be masked in all public areas. They can’t hang in resident’s rooms if they have a roommate. There still are a welter of confusing limitations on visitations that continue to this day.
Plexiglass barriers still all over nursing homes. Capacity limit signs on elevator and breakroom doors. Chairs in the waiting areas still look like this:


So, to be fair, the environment of care has shifted from the utter, batshit-insane times of early 2020 where our residents were locked up completely from the outside world, and incredibly sad things like prison-like “window visits” were instituted while they simply sat and waited, ostensibly, for vaccines to be developed and issued so they could, well, get back to normal.
But, as you can see - we are very much not back to normal in my nursing home, and to varying degrees (probably likely generally worse in blue areas) this is how long-term care currently looks for nursing homes across the USA, if not many parts of the world.
Residents in my nursing home still get constant reminders that they are in an emergency and that there is danger everywhere.
Residents are not able to see the faces of their caregivers, and due to masks and often face shields, struggle to understand them.
Residents are still not able to see family members faces in public.
I don’t want to repeat myself - but the fact is, nursing home patients live in a world which is still basically like 2020 was for most of us, if not worse. Things are not back to normal for them.
Urgency of Normal for Nursing Homes?
Was having a discussion the other day with a very influential figure in the Urgency of Normal movement, Dr. Scott J Balsitis - and I found him to be a really lovely, pleasant man who made me feel right at ease when speaking with him.

But as I ‘talked shop’ with him about his history of advocacy with his colleagues (Drs. Lucy McBride and Tracy Beth Hoeg), and how over the last year or so they fought to successfully push back on what looked to be an unacceptable situation developing in US schools (that of possible forever masking, and a future of ongoing, intermittent school closures) - I got a sense in Scott a sense of steely determination.
He, Lucy, Tracy and others had to fight a fight from a number of fronts when it came to reopening schools and liberating children from “school prison,” a prison of shutdowns, lockdowns, social distancing, masking, and other potential worse abuses.
There was the public fight that was often fought by the very photogenic and poised Dr. McBride, who stood for TV interviews and testified in front of legislators:
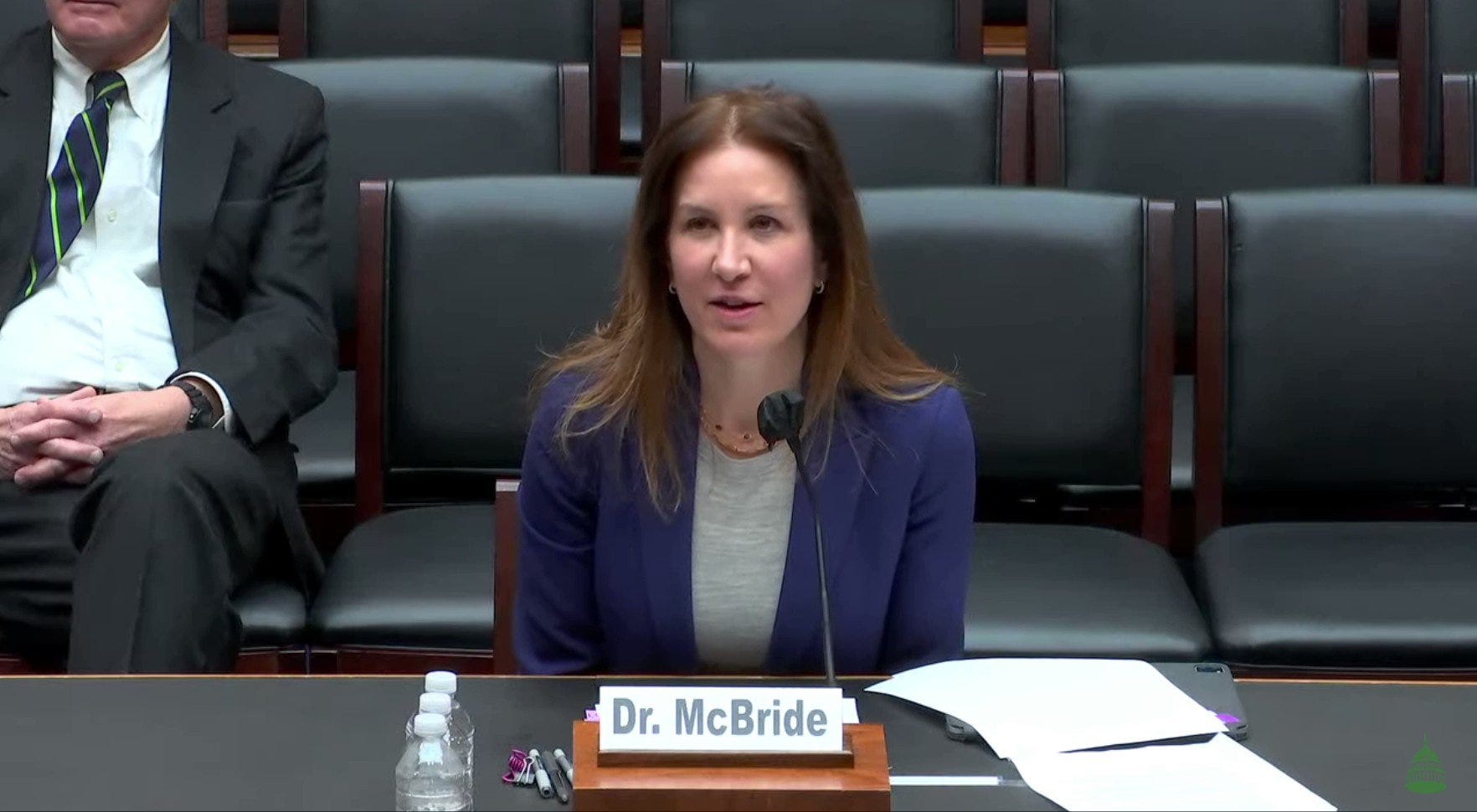
The thing was though, although Dr. Lucy McBride, who is fantastically well-spoken and photogenic, was able to bring to bear convincing data and science to her argument for reopening schools and getting masks off of children, it wasn’t enough for her to get in front of cameras and bring all of the data and science in.
Scott explained to me, the real battle was fought in terms of finding where the “lever of power” was, as it were, and how these levers could be successfully moved.
In the case of schools - it was the school administrators, the local decisionmakers who hire and fire employees. However, as Scott explained to me:
“…going against the CDC exposes (the school administrators) to criticism and professional risk, while going along with the CDC insulates them: if the CDC is wrong, that's the CDC's fault, not theirs…. In those cases, it will NEVER matter how good our scientific arguments are, because science isn't on the administrator's mind.”
So while it was these administrators who proved to be the actual levers of power - it was only by mounting large-scale protest and letter-writing campaigns by parents that these school administrators became levers that could actually be moved.
While Scott, Tracy, and others had the science on their side, they needed to get the social networks that mattered to these school administrators to actually start to make some noise and incentivize them into action: in other words, the parents and communities within which these school administrators worked. As Scott went on to say:
… (by) convincing a large majority of local administrators that school disruptions were harmful (or giving them the data to articulate what they already knew/suspected), we forced the CDC into an untenable position: they could either adjust their position to one that was both more scientific and better acknowledges the importance of individual values and choices, or they could be left looking increasingly irrelevant and out of touch.
Why did it work?
Well remember that despite all of the national attention that the plight of schoolchildren get in popular media and from politicians, in the United States at least, a majority of school funding still comes from local property taxes, parcel taxes, and local school bonds. Mostly state and overwhelmingly local funding, with only about 8% of any given public school funded with Federal dollars.
This has direct implications for campaigns like those that Scott, Lucy, Tracy and others led to reopen schools, get masks off of kids, and get them to back off of these vaccine mandates.
To be fair to these school administrators (and Scott wanted to make sure I pointed this out) - most of them didn’t need to be dragged kicking and screaming into reopening the schools and unmasking the children. Most of these administrators were reasonable people who saw with their own eyes that COVID-19 was not a risk for children and the risk to teachers and administrators was manageable.
What was needed was simply a way to give these administrators a reason to do what they did (and many, eagerly) - in the end, to act on behalf of the community and the families and children whom they were ultimately accountable to.
Great! Can we do this in nursing homes?
The Fulcrum of Power is Different in Nursing Homes based on How Nursing Homes are Funded
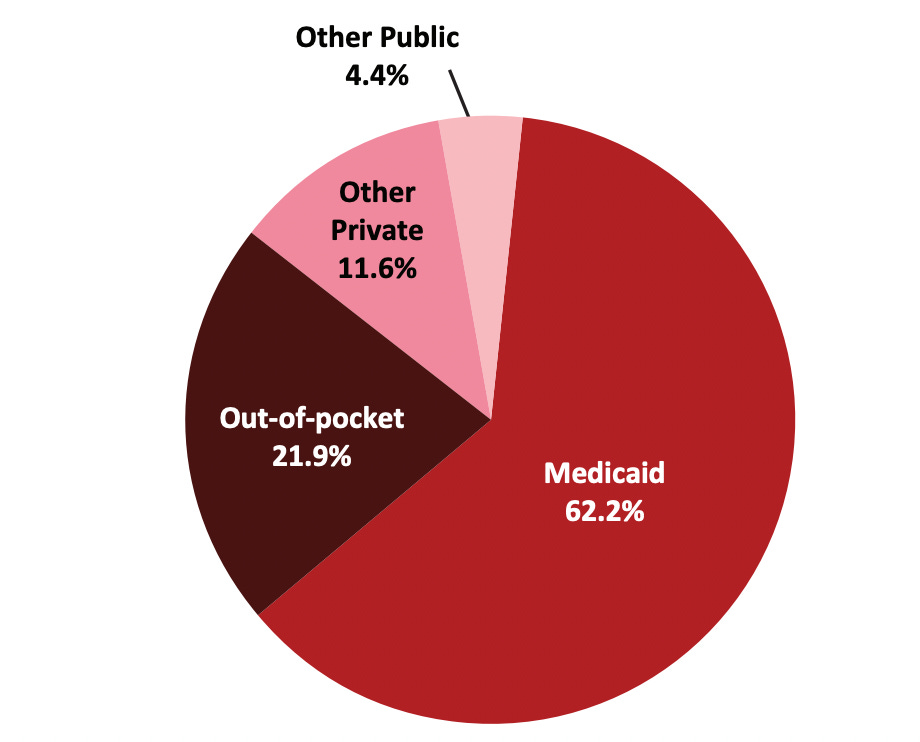
In community skilled nursing facilities, the funding sources (and therefore, the incentives) are almost completely flipped on their head.
For the overwhelming majority of the dollars (approximately 2/3) spent in community nursing homes, the funding comes from a mix of Medicare and Medicaid dollars, both of which are federally-funded programs (in the case of Medicaid, the program is nominally administered by the state but the Federal Government dictates, for the most part, how the money is spent).
This alone means that the nursing administrators / Directors of Nursing (DONs), the ones who make the hiring and firing decisions, their salaries and the salaries of those they employ overwhelmingly don’t come from local dollars - they come from the federal government.
Again, remember - incentives matter. As much as we all want to do the right thing for our residents and their families, it becomes very important who is paying our paycheck.
Accrediting Agencies and Regulations Complexify Things Further and Make the Levers of Power in Nursing Homes More Opaque
I've said many a time over the years that elder care, and specifically skilled nursing care in the United States is one of the most heavily regulated industries on earth.
Not only all of our employees (excepting, perhaps, the food service and janitorial staff) subject to exacting government occupational licensing standards, and not only are we subject to all of the normal regulatory policies you’d expect at a hospital, nursing homes are required to adhere to the dictates of the Minimum Data Set, or MDS - which is a very lengthy assessment which is required to be completed on all nursing home residents of all US nursing homes, every quarter, and covers domains like eating, sleeping, mood, cognitive status, behavior, and governs the care planning process, and also determines how nursing homes are funded, or paid, by Medicare & Medicaid.
I could write several blog posts about MDS and barely even scratch the surface of an introduction.
Finally - there are the accrediting agencies, like most famously the Joint Commission on Accreditation of Healthcare Organizations (known as JHACO, or often just “Joint Commission), and also groups like the Long Term Care Institute, which specializes in nursing home accreditation.
Again, too much to summarize in one article - but the point is that long term care is subject to a confusing welter of centralized & largely federally monopolized funding sources, accrediting agencies, in an otherwise very highly regulated sector of the medical system.
Replicating the “Levers of Power” Approach Scott Utilized for the Urgency Of Normal in Long Term Care?
Yeah, I hate to sound pessimistic - but I think this is why simply trying to replicate the Urgency of Normal’s “finding the lever of power and pressuring it” approach may not work in the long term care industry.
More than anything, a letter writing or protest campaign targeting DONs and nursing home administrators won’t likely be persuasive the way these letter writing campaigns and pressure campaigns worked in schools - and it’s because unlike school officials, who are largely funded with local dollars (and thereby answerable to the local community - despite what the CDC may say), the funding situation is completely turned on it’s head in LTC.
Also - let’s be honest. Family members of older people in long term care are not the same as parents of children. Sadly, a lot of wives and husbands of older adults are older and frail themselves, and aren’t exactly savvy or energetic when it comes to advocacy.
Older GenX sons and daughters, already “double caregivers” themselves (caring for older kids at home, sometimes granchildren of their own) don’t exactly have the time to mount a spirited defense of the rights of their loved ones stuck in nursing care.
All of this makes for a perfect storm of inaction and ennui that means the bureaucratic focus on emphasizing masks, quarantines, testing, plexiglass, the social distancing signs - e.g., manufactured fear - is likely to persist that much longer for the environment of care of older people in facilities.
So what’s the answer?

I may be wrong and maybe we could do an “Urgency of Normal” type campaign with nursing homes if we were able to drum up the proper amount and degree of advocacy that Scott, Lucy, and others at UoN were able to drum up.
But if not - I don’t think the cause is totally lost. In my next Substack post in a couple weeks, I’ll explain why. Stay tuned!
While not as dire in my area for LTC I despair of EVER getting rid of masks for caregivers, nor the forced weekly nasal rapes regardless of symptoms for EVERYONE when there is an outbreak. Nevemind even CMS doesn't recommend this anymore-the LTC corporate overlords have deemed it necessary to cover their own asses. At least my residents can go out, aren't quarantined upon return etc. But we are now seeing a wave of deaths from the imposed restrictions previous that sharply increased depression leading to severe increase in frailness and worsening of their disease states. MANY residents-who were functioning, relatively happy resident prior to 2020-have expressed their desire to just die to be done with it - they OVER the constant threats of everything they have left to live for being taken away on a whim. Keep in mind most have "survived" covid of 2020, 2021, 2022 with nary a sniffle by this point, and have been jabbed 4-5 times-each with promise of "normality" returning.
FAMILIES need to SUE CMS for intentional HARM, neglectful policies and need the MEDIA local and national to start spotlighting this-starting with fear porn Walensky herself-we need reporters who are NOT AFRAID of actually asking the hard questions and follow ups and push her and st fauci into corners to make fools of themselves and keeping that on nightly news for weeks (like they do with the USELESS case counts of ONLY covid)
Myself-I am actively looking to get out of my field of 20+ years as I cannot stand the thought of masking for rest of my years until retirement when rest of society doesn't have to anymore.
Thank you for sharing and for being a voice for the voiceless. This madness has to end, but I think you are correct and if money is involved, there’s no incentive for it to end. It’s all about control. Sadly, medicine as a whole stopped being about the patient years ago, and LTC communities are no different. It used to be what is in the best interest of the patient. First do no harm. Those aren’t even considered now. It’s going to get a lot worse before it gets better. As long as the government continues to hold the purse strings, they will control everything.