


The Long Shadow of the Coronapanic: The LTC Nursing Shortage of 2024 and Beyond
The Coronapanic caused a massive nursing shortage in LTC. Unlike in other practice areas of nursing (ICU nursing, pediatrics, etc.), LTC nursing has yet to recover from this. I'll explain why.

I am not intimately familiar with the American Health Care Association, or AHCA. I can say that they have been around since 1949 and appear to function basically as a trade group for the long-term care industry, representing around 14,000 different non-profit and for-profit long-term care facilities, along w/ assisted living facilities, and facilities that serve the developmentally disabled.
For sure, they are an advocacy group - so they are advocating for better funding such as via more generous Medicare and Medicaid funding for their members, and in that sense they are political.
But, relative to a lot of professional guild or trade protection groups (like, say, the American Academy of Pediatrics, or the American Nursing Association, who both lept feet-first into woke politics and the transgender craze), they are refreshingly, boringly unbiased and “un-woke.”
With that setup, wanted to refer you to this press release from the AHCA, which I stumbled across when I was combing through Perplexity.AI:
Basically, US long term care is in serious trouble.
We all know there have been some longstanding issues w/ nursing shortages across the industry (long term care, assisted living, ICU nursing, ER nursing, pediatrics, etc). This feature article in the Atlantic Magazine from 2016 highlights the issue, and I think it’s fair to say most of us have heard the entreaties for young people to do nursing careers for quite some time.
Then COVID happened.
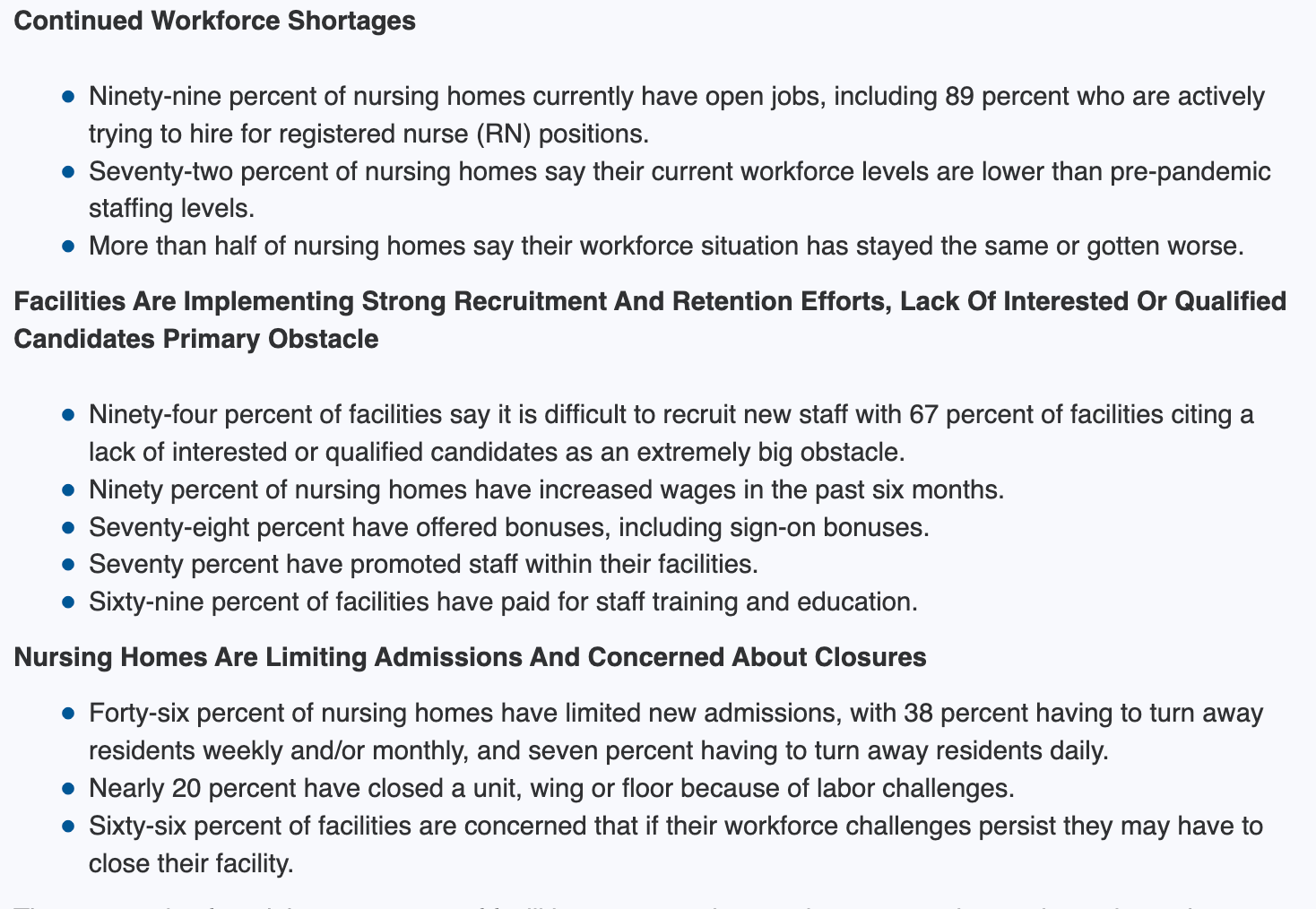
I can’t speak to what happened outside of my little sphere (long term care skilled nursing), but my understanding is that it’s was largely devastating to the entire industry. The AHCA report bears this out - with these as highlights:
So why is this going on?
Even before the Coronapanic - I’ve heard it said that long term care is a very “special” industry to work in. We are a special kind of people. The pace in long term care is different than ER or acute / ambulatory care. It’s not like working in a clinic. Although what we do often overlaps with the kind of work done in subacute or “short stay” nursing care (e.g., which involves intensive rehab with the aim of getting a resident home), the overall philosophy and rehabilitative aim is critically different than that of any other place in the medical system.
Older people who are living in skilled nursing facilities are, for the most part, going to live where we work, this is their homes. They will not be cured of what brought them to us. When we offer them rehabilitation - it’s largely for the purpose of slowing declines in functioning, possibly arresting further decline, as opposed to restoring key function that might get them back into the community.
Quality of life, actually, is the biggest thing.
The nursing staff and other clinical staff at my nursing home get to know our residents. They become like family, and vice versa

When the coronapanic happened, it was, like I like to say, a nuclear bomb on long term care.
Masks everywhere. Face shields. We put masks on residents. No more congregate dining. Family visits banned for weeks, and then absurdly cruel “window visits” as an insult of a replacement - which, for our 50-70% of residents with dementia, simply added insult to injury.
The fact is that the coronapanic and all of the absurd and cruel rules that were imposed on us, so obviously completely counter to the traditional care philosophy in long term care nursing - that of quality of life, comfort, and striving for home-like conditions, it turned my nursing home and thousands of others across the country into depression factories, where residents lost function and the will to live.

So think about this from a career long-term care nurse’s perspective.
You’ve worked in long term care for years, perhaps decades. Suddenly, your job is no longer life-affirming. You become a jailer, an emotional torturer of your residents. Arbitrary, absurd, and constantly-shifting cruel rules to “defeat a virus” become the norm.
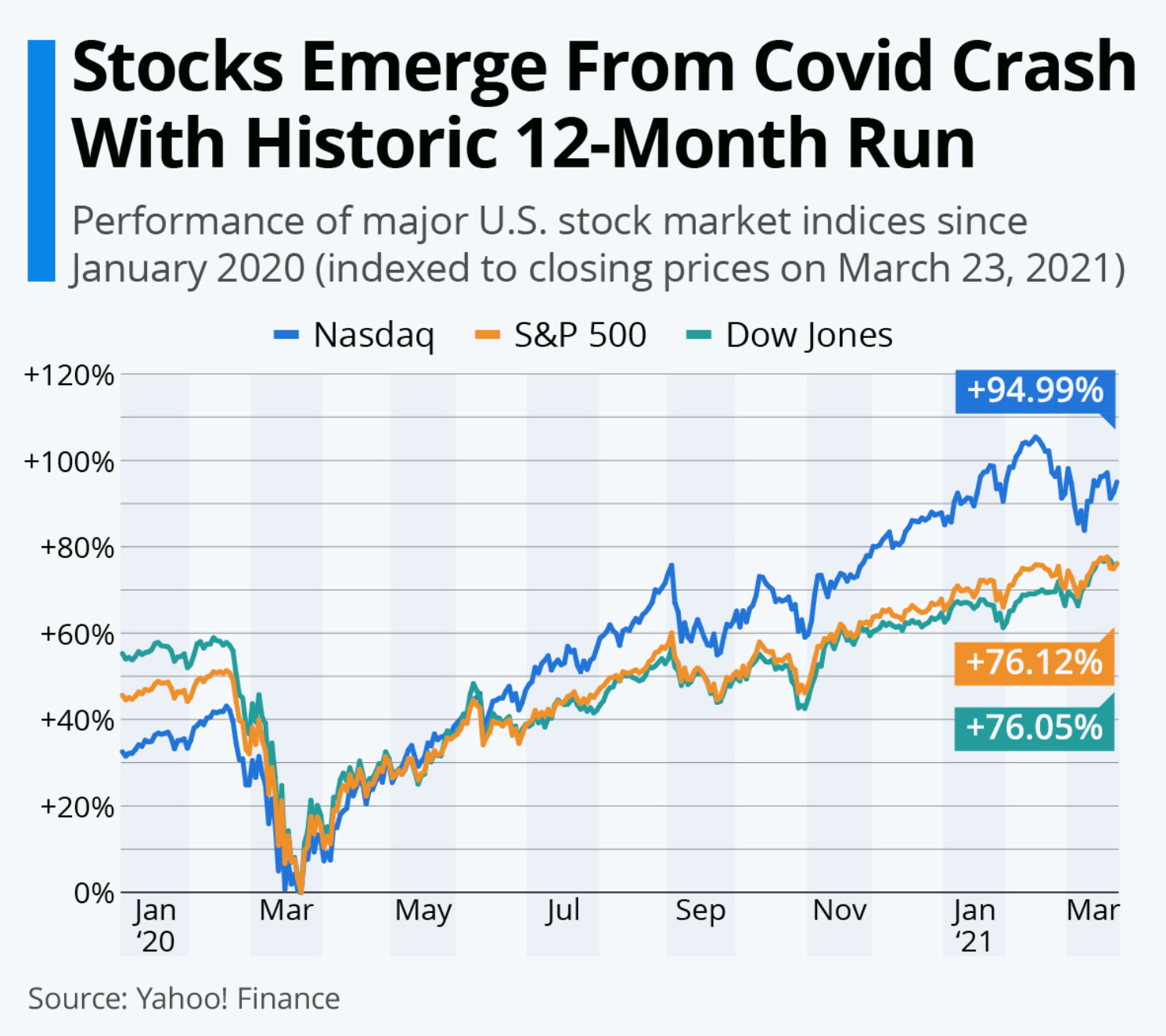
Also, if you are an experienced nurse and you’ve contributed to a retirement account, you see your 401K balance more stuffed than ever.
So, nursing staff - particularly the exact ones we would want to retain in LTC - said “screw this, we’re outta here! We don’t want to stay here and feel like elder abusers!” - and they left, and never came back.
I think that there’s a crisis afoot in terms of elder care. Even prior to the coronapanic, the long-term care market in the United States was highly dysfunctional. The long term care insurance market is largely broken.
Now, it’s even worse. What is anyone doing to fix it? It’s a combination of decades of neglect, virtue-signalling pretend fixes, and the destructive effects of an irresponsible, if not criminal mass public health panic fomented by bad actors who have, as of yet, not been held accountable - and moreover, many of the policies and practices that were put into place by the coronapanic are still there.
For example, at my nursing homes in my regional network - even though it’s a lot of very cursory chin-masking at this point, we are still required to mask around our residents. It’s insane. When will this stop?
Thank you for bringing attention to the critical condition of LTC world.
Re: staffing - RNs when I see them now are in management or admin , the LPNs are unit managers and sometimes do med passes; the med techs usually pass meds and then the caregivers provide direct care. The med tech and caregiving staff are typically here today and gone tomorrow, usually when they get tired of being mandated for extra hours and realizing fast food restaurants don’t mandate and don’t require back-breaking incontinent or other repetitive heavy assists.
Never mind that LPNs by license aren’t supposed to assess, the RNs do that, but if you can’t get RNs, then what? Who decides when a patient needs an as-needed medication if there is no one who can assess due to their license? Or assesses change of status? Or when staff is so short the assessments aren’t done and those PRNs just don’t get given?
Most LTC where I go rely heavily on African immigrants, who like Americans, some are excellent at their jobs and others not so much. Heavy accents, lack of understanding of the culture of elderly Americans and mask wearing combine to create communication problems which only exacerbate the stressors of being in a night-noisy environment with crappy food that is served cold and late.
None of it is good. Now new CMS regs are starting which will increase the time and hassle required for providers to get through their day. Mandatory gradual dose reduction, calling family with every single med change not just when discussing adding something new or changing plan of care promises to lengthen the work day even more.
I’m not sure what to think anymore. It sure is a different world in LTC since the Coronapanic and it is in serious trouble.
I appreciate you bringing attention to this. Low pay, poor working conditions and lack of support have contributed to excessive burn out that has come to a head. Working with patients who are abusive (physically and verbally), admins that make decisions based on numbers and not reality, lack of support (true support, not “pizza Fridays” and the occasional paid for lunch), lack of training for staff and failure of accountability for fear of becoming even more short staffed have many wonderful nurses asking themselves “why bother?” and moving on to less stressful jobs. The sheer cost of long term care is excessive- do the people who actually provide the hands on care see a fraction of what is charged? Not likely- it goes to “administrative costs.” So who can blame those people for leaving? I also blame the medical profession- interventions aimed at just keeping people alive instead of looking at quality of life. I started noticing this long before Covid- the lack of palliative care, hospice options and spiritual guidance have eroded our system to this point. I don’t have the answer, but I can see that this is a situation that will not end well. Sadly a lot of family members too are facing this unprepared. Being told a family member needs to go into a nursing home because they can’t live alone and/or they need medical care but no places are available- then what? Quality of life is declining and people are living longer. We should look at what other countries (who are successful navigating this phase of life) and implement what they are doing. But we won’t- America likes to reinvent the wheel and kick the can down the road for someone else to deal with. Guess what? The end of the road and the cliff are coming.